
Neglect Practice Guidance
Introduction
This guidance has been written in line with the Working Together to Safeguard Children: A guide to inter-agency working to safeguard and promote the welfare of children. The practice guidance has also considered research including reports by DfE, Missed Opportunities: indicators of neglect – what is ignored, why, and what can be done? November 2014, and DfE, The impacts of abuse and neglect on children; and comparison of different placement options, March 2017
The document includes the definition of neglect; indicators of neglect; links to other useful information and research into the impact of neglect on children. The practice guidance is also designed to help practitioners to identify, assess, question and consider all the risk factors within the context of neglect using tools such as the North Yorkshire Framework for decision-making: Right Help, at the right time by the right person and adopting a strength in relationships practice model approach.
Scope
This guidance is for all professionals who work with children and young people in North Yorkshire.
Legislation and Standards
- Working Together to Safeguard Children
- Children and Families Act (2014)
- Children Act (2004)
- Children Act (1989)
- NICE (2009)
Policy Statement
The guidance will provide an overview of:
- Risk indicators to establish if a child is being neglected in accordance with the Working Together, definition
- Assessment method to aid the practitioner to identify if the child is being neglected
Latest research into the impact of neglect on children to assist with practitioners having a fuller understanding of the issues
What is Neglect?
The definition of Neglect is:
‘The persistent failure to meet a child’s basic physical and/or psychological needs, likely to result in the serious impairment of the child’s health or development. Neglect may occur during pregnancy as a result of maternal substance abuse. Once a child is born, neglect may involve a parent or carer failing to:
- provide adequate food, clothing and shelter (including exclusion from home or abandonment);
- protect a child from physical and emotional harm or danger;
- ensure adequate supervision (including the use of inadequate care-givers); or
- ensure access to appropriate medical care or treatment.
It may also include neglect of, or unresponsiveness to, a child’s basic emotional needs’.
Working Together to Safeguard Children .
- Nutritional neglect is usually associated with inadequate food for normal growth leading to “failure to thrive’” (now referred to as ‘faltering growth’). Increasingly another form of nutritional neglect from an unhealthy diet and lack of exercise can lead to obesity, which increases the risks to health in adulthood
- Emotional neglect Emotional abuse is the ongoing emotional maltreatment or emotional neglect of a child. It’s sometimes called psychological abuse and can seriously damage a child’s emotional health and development. Emotional abuse can involve deliberately trying to scare or humiliate a child or isolating or ignoring them.
- Educational neglect includes carers failing to comply with state requirements, but also include the broader aspects of education such as providing a stimulating environment; showing an interest in the child’s education and supporting their learning including that any special educational needs are met.
- Physical neglect refers to the dirty state of the home, lack of hygiene, lack of heating, inadequate and/or broken furniture and bedding. It may include poor or inadequate clothing, which mark a child as different from his peers resulting in isolation or bullying. It also refers to a lack of safety in the home, exposure to substances, lack of fireguard or safety gates, and exposed electric wires and sockets.
- Failure to Provide Supervision & Guidance refers to the carer failing to provide the level of guidance and supervision to ensure that the child is physically safe and protected from harm.
In addition to Howarth (2007) there are the following categories and indicators of neglect which are based on research (Crittenden 1999, cited in NCH Action for Children, ‘Action on Neglect’ 2013) and these too may help practitioners to plan and manage neglect cases. The research suggested that neglect can be grouped as follows:
- Disorder Neglect
- Emotional Neglect and
- Depressed Neglect
Detailed below is a table which provides examples of what these forms of neglect may look like, possible solutions and cautionary words for practitioners. It must be noted that it is not possible to create a comprehensive and exhaustive list of indicators of neglect as these will be presented in very different ways according to the family and child/ren.
Neglect of a Childs Health Needs:
The neglect of a child’s health needs can lead to long and/or short term impact on their health and development and in extreme cases can lead to a child’s death.
Failing to meet a child’s health needs may take several different forms, including:
- Delay in in seeking timely and appropriate medical care for a serious health problem that any reasonable person would have recognised as needing professional medical attention
- Failure to ensure a child receives medication or treatments prescribed by a registered health professional
- None or inconsistent adherence to recommended therapies for example physiotherapy
- Nonattendance or inconsistent attendance at health appointments to monitor, or to receive treatment for an existing health issue
Dental Neglect:
Dental neglect is defined as:
‘…the persistent failure to meet a child’s basic oral health needs, likely to result in the serious impairment of a child’s oral or general health or development‘ British Society of Paediatric Dentistry
Dental neglect often results in widespread dental caries and frequently leads to multiple dental extractions. Dental caries will often result in significant dental pain and impact on the child’s sleep patterns, nutritional status and general health status. Multiple dental extractions often impact on a child’s speech and their social and emotional development.
Each case should be assessed individually in the context of the child’s medical history and developmental stage, as well as factors such as access to dental treatment. However, particular cause for concern would include: missed appointments for necessary treatment and failure to complete planned treatment.
Using the term ‘Was not brought’ instead of ‘Did not attend’:
The term ‘Was not brought’ (WNB) as opposed to’ Did not attend’ is preferred and used by health professionals across North Yorkshire as it encourages us to:
- Think about the situation from the child’s perspective:
- Consider how the parents/ carers are responding g to the child’s health needs
- Identify any impact on the child’s wellbeing
- Plan what support would help the child to receive the health care they need
- Consider whether we need to share safeguarding information with other health or social care professionals.
Questions to ask when considering the possibility that a child’s health needs are been neglected:
- Do the parents/ carers understand the specific health needs and treatments required for their child?
- Are there multiple conflicting appointments?
- Are the appointments been sent to the correct address?
- Are there any literacy issues impacting on the parent’s ability to prioritise appointments?
- Are there any issues with transportation to appointments or to pick up medication?
Indicators
| Indicators: Disorder Neglect (driven by chaos and crisis) | Possible Solutions/ Interventions | Practitioner Caution |
| Families have multi-problems and are crisis ridden Care is unpredictable and inconsistent, there is a lack of planning, needs have to be met immediately Parent appears to need/want help and professionals are welcomed, but efforts by professionals are sabotaged by the parent Generational abuseChildren become overly demanding to gain attentionFamilies constantly recreate crisis, because feelings dominate behaviourParents feel threatened by attempts to put structures and boundaries into family lifeInterpersonal relationships are based on the use of coercive strategies to meet needFamilies respond least to attempts by professionals to create order and safety in the family | Feelings must be attended to in order to develop trust, express empathy and reassurance, be predictable and provide structure in the relationshipMirror the feelingsGradually introduce alternative strategies to build coping skills Support will be long term | Practitioner can become easily absorbed into the family, resulting in over-optimism and feeling positive about minimal change when in fact the needs of the child remain unchanged |
| Indicators: Emotional Neglect (absence of empathy, not good at forming relationships) | Possible Solutions/ Interventions | Practitioner Caution |
| Opposite of disorganised families where focus is on predictable outcomesFamily may be materially advantaged and physical needs may be met but no emotional connection madeChildren have more rules to respond to and know their role within the familyHigh criticism/low warmthParental approval/attention achieved through performanceChildren learn to block expression/or awareness of feelingsThey often do well at school and can appear overly resilient/competent mature They take on the role of care giver to the parent which permits some closeness that is safer for the parent Children may appear falsely bright, self-reliant, but have poor social relationships due to isolationParent may have inappropriate expectations in relation to the child’s age/developmentParent will feel threatened by any proposed intervention | Parents need to learn how to express feelings/emotionally engage with the child Children will benefit from socially inclusive opportunities Help parents to access other sources of support to reduce isolationChild needs support from non-abusing family member | Practitioners find this type of family difficult to work with because of the lack of understanding of emotional warmth by the parent. Removal of the child will reinforce their feelings of rejection As families may appear successful, there is less likely to be professional involvement |
| Indicators: Depressed Neglect (withdrawn and dulled parental characteristics, unresponsive) | Possible Solutions/ Interventions | Practitioner Caution |
| Parents love their children but do not perceive their needs or believe anything will changeParent is passive and helplessParent is uninterested in professional support and unmotivated to change Parental presentation is generally dull/withdrawn Parents have closed down awareness of children’s needsParents may go through the basis functions of caring, but lack responsiveness to child’s signalsChild is likely either to give up through lack of response and become withdrawn/sullen, or behaviour may become extreme | Children benefit from access to outside stimulation e.g. day care Parents unlikely to respond to strategies which use a threatening approach that requires parents to learn new skillsConsider if the parent may be depressed and if so encourage them to make an appointment with their GPEmphasise strengths Parental education needs to be incremental and skills practised and reinforced over time Support likely to be long term | Often linked to substance misuse or mental health problem. Practitioners need to be realistic about the level of change. Easy for practitioners to get caught up in the sense of ‘hopelessness’. |
Specific considerations for the neglect of adolescents
It is important to hold in mind that child neglect not just for young children but profoundly impacts the significant age range of 11-18 years old. Recent Serious Case Reviews claim that adolescents were found to be the group most likely to be the subject of a case review after that of infants (Brandon et al, 2020).
The pandemic has compounded the already complex area of care and support for adolescents.
These include changes and challenges to social activities, mental health, internet activity, increased isolation, and decreased motivation. Additionally, for some adolescents lockdown compounded the abuse and neglect they were already experiencing. There is a requirement to consider the needs of this group in a more specialised way to halt a social pandemic in young people. Kobulsky et al, (2021) conducted a longitudinal study of child abuse and neglect of 1050 adolescents aged 16 and 18. Risk behaviours of substance abuse, sexual and emotional and behavioural issues and delinquency, were highlighted which contributed to a 5 factor model of adolescent neglect. The areas are:
- exposure to risk
- inadequate monitoring
- inattention to basic needs
- the permitting of misbehaviour, and
- inadequate support.
It is possible adolescents may have suffered with this, experiencing years of neglect and emotional distress leading to false evaluations of their resilience, partly from themselves, and partly from others (parents and workers). Professionals may have an awareness of some of the behaviours that adolescents experiencing neglect may display. Some of these include an increased vulnerability towards sexual abuse, inability to develop secure attachment habits, risk taking in the community, poor engagement with education, poor mental and physical health, increased risk of accidents, and a lesser ability to holistically develop in the same way other children develop.
Brandon, M. et al (2020) Complexity and challenge: a triennial analysis of SCRs 2014-2017: final report. London: Department for Education.
Kobulsky, J.M., Villodas, M., Yoon, D., Wildfeuer, R., Steinberg, L. and Dubowitz, H. (2021). Adolescent Neglect and Health Risk. Child Maltreatment, p.107755952110497
https://journals.sagepub.com/doi/abs/10.1177/10775595211049795
Next Steps
All agencies should consider this guidance alongside the Framework for decision-making: Right Help, at the right time by the right person; these should be used as a guide to identify how children’s needs might be met across universal, early help, targeted prevention and intensive/acute services.
North Yorkshire Children and Families Multi-Agency Screening Team (MAST) is a single point of contact for all referrals relating to safeguarding, Prevention, Disabled Children’s Services and HDFT Health Child Programme.
All referrals should be sent to the Multi-Agency Screening Team.
Agencies should complete the Universal Referral Form for Children and Families Service and send to:
If you have a concern that a child or young person has suffered or is likely to suffer significant harm or would like to discuss the referral then please contact the Customer Resolution Centre on 0300 131 2 131.
In cases where there is immediate danger to a child or young person you should call 999 and request, the assistance of Police without delay.
The professionals in the Multi-Agency Screening Team work together to ensure the right services are provided to the child and their family at the right time. On receipt of the referral the MAST will:
- Undertake multi-agency screening of the referral
- Share information from each agency
- Consistently use the Signs of Safety approach and ensure a outcome for that referral within 24 hours
- Ensure a response to the referrer within 5 working days
For further information on the referral process please see:
- NYSCP Practice Guidance and One Minute Guides
www.safeguardingchildren.co.uk/professionals/procedures-practice-guidance-and-one-minute-guides - Making a Referral One Minute Guide
https://www.safeguardingchildren.co.uk/professionals/procedures-practice-guidance-and-one-minute-guides/making-a-referral/ - Referrals to the Children and Families Service Using the Updated Universal Referral Form One Minute Guide
www.safeguardingchildren.co.uk/professionals/procedures-practice-guidance-and-one-minute-guides/referrals-to-children-and-families-service-using-the-updated-universal-referral-form - Using the Universal Referral Form One Minute Guide
https://www.safeguardingchildren.co.uk/professionals/procedures-practice-guidance-and-one-minute-guides/using-the-children-and-families-universal-referral-form/ - Worried about a child? Make a Referral
www.safeguardingchildren.co.uk/about-us/worried-about-a-child/
Talking to children and their families about the referral
It is good practice to be open and honest at the outset with parents and carers about the concerns, the need for the referral and information sharing between agencies. All reasonable efforts should be made to inform parents prior to making of the referral. A referral should not be delayed if you are unable to discuss your concerns with parents.
Concerns should not be discussed with parents/carers where this would put the child at significant risk of harm. If you need to seek advice then please contact the Customer Resolutions Centre on 0300 131 2 131.
Assessment
It is recommended in the study by Department for education DfE, November 2014 for practitioners to undertake an assessment for neglect by considering three key areas:
- Description of current state and identification of any current indicators of neglect:
- Exploration of persistence of indicator – is this something that happens frequently /all the time/ never been noticed before?
- Assessment of the current functioning of the child and of the family.
- Review of underlying risk factors incorporating a previous history of:
- The child and of each parent/caregiver.
- Professional involvement and the family’s response to this.
- Assessment of the parents’ capacity to change:
- This can only be tested as part of the parental response to sound, supportive intervention which focuses on social and environmental risk factors and neglectful parent-child interactions.
Good Practice – Ofsted’s research report, March 2014 found that practitioners had better assessments where they adopted a standardised, structured approach and one that social workers valued which had clear theoretical foundations. The examples recognised were Signs of Safety (which is an approach underpinned by North Yorkshire) and the Graded Care Profile.
Case Management of Neglect
Neglect cannot purely be seen solely in the moment and free of context. In discussing significant harm it is possible that it can be suggested or low-lying with a likelihood of becoming more pronounced over time and we mustn’t minimise the impact of cumulative neglect. A significant percentage of children who were the subject of serious case reviews due to incidents and deaths were known to agencies and experiencing long term neglect. Improvements to the management oversight of neglect cases may decrease drift and delay and an increased focus could minimise tragic outcomes. This may also provide professionals with the ability to take a step back and review cases alongside their own values and biases. Research by the University of East Anglia in 2013, analysed 645 serious case reviews in England between 2005 and 2011, finding that 59% of children who died or were seriously injured were on a child protection plan for neglect during or prior to the injury/death.
Professionals may struggle with:
- Lack of challenge.
- Loss of focus on the lived experience of the child,
- Issues of de-sensitisation to the effects of neglect
- Loss of focus due to chaotic nature of a neglect case
- Uncertainty based on the objectivity of managing the case to resolution
- Identifying and challenging disguised compliance
Improvements may include ways of addressing the wider managerial issues to provide support and improve the management of cases.
- Increased effective decision making
- Timely responses aided by reviewed regularly supervision
- Multi-agency professional meetings
- Regular appraisal of the working relationships between the family and those working alongside them to ensure that the measured balance of challenge and support is upheld towards the family
ESCB Policy & Procedure Sub-committee. (2017) Neglect Multi-Agency Practice Guidance For thoseworking with children, young people and families in Essex. https://www.escb.co.uk/media/1517/escb-neglect-practice-guidance-2017-finaldoc.pdf.
DFE (2020) Safeguarding system needs to do more to protect teens and infants from abuse and neglect. A report by the Child Safeguarding Practice Review Panel calls for improvements to the safeguarding system.https://www.gov.uk/government/news/safeguarding-system-needs-to-do-more-to-protect-teens-and-infants-from-abuse-and-neglect.
Escalation Process
If a professional disagreement occurs between agencies regarding the management of a particular case, the NYSCP has practice guidance on ‘Professional Resolutions’. The practice guidance provides an overview of how agencies should address their concerns using a seven stage approach. The practice guidance is available from the NYSCP website:
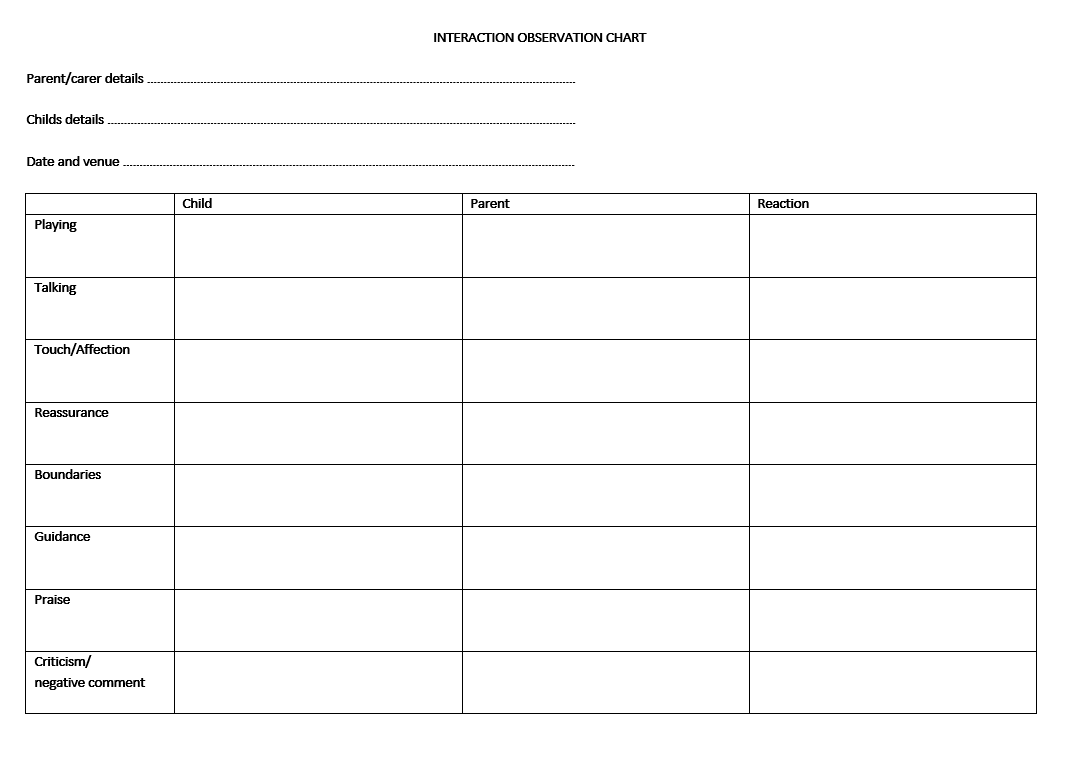
The interaction observation chart maybe a useful tool for any professional as part of their assessment.
INTERACTION OBSERVATION CHART
Parent/carer details …………………………………………………………………………………………………………………
Childs details ……………………………………………………………………………………………………………………………
Date and venue ……………………………………………………………………………………………………………………….
| Child | Parent | Reaction | |
| Playing | |||
| Talking | |||
| Touch/Affection | |||
| Reassurance | |||
| Boundaries | |||
| Guidance | |||
| Praise | |||
| Criticism/ negative comment |
(Adapted from South Gloucester LSCB, Child Neglect Toolkit for Practitioners)
USEFUL RESOURCES (the below list is hyperlinks to the original online sources)
Neglect and Serious Case Reviews: A report from the University of East Anglia commissioned by NSPCC
Framework for decision-making: Right help, at the right time by the right person
South Gloucester Safeguarding Children Board, Child Neglect Toolkit for Practitioners.
University of Sterling research on neglect
Brandon, M. et al (2020) Complexity and challenge: a triennial analysis of SCRs 2014-2017: final report. London: Department for Education.
Kobulsky, J.M., Villodas, M., Yoon, D., Wildfeuer, R., Steinberg, L. and Dubowitz, H. (2021). Adolescent Neglect and Health Risk. Child Maltreatment, p.107755952110497
Working Together to Safeguard Children
ESCB Policy & Procedure Sub-committee. (2017) Neglect Multi-Agency Practice Guidance For those working with children, young people and families in Essex.
https://www.escb.co.uk/media/1517/escb-neglect-practice-guidance-2017-finaldoc.pdf.
DFE (2020) Safeguarding system needs to do more to protect teens and infants from abuse and neglect. https://www.gov.uk/government/news/safeguarding-system-needs-to-do-more-to-protect-teens-and-infants-from-abuse-and-neglect.
NYSCP Practice Guidance and One Minute Guides
www.safeguardingchildren.co.uk/professionals/procedures-practice-guidance-and-one-minute-guides
Making a Referral One Minute Guide
www.safeguardingchildren.co.uk/professionals/procedures-practice-guidance-and-one-minute-guides/making-a-referral
Referrals to the Children and Families Service Using the Updated Universal Referral Form One Minute Guide
www.safeguardingchildren.co.uk/professionals/procedures-practice-guidance-and-one-minute-guides/referrals-to-children-and-families-service-using-the-updated-universal-referral-form
Using the Universal Referral Form One Minute Guide
www.safeguardingchildren.co.uk/using-the-children-and-families-universal-referral-form
Worried about a child? Make a Referral
www.safeguardingchildren.co.uk/about-us/worried-about-a-child
Framework for decision-making: Right Help, at the right time by the right person
Page reviewed: December 2024

 View all our news
View all our news